The Big Question: Is changing behaviour now the key weapon in the fight against Aids?
Your support helps us to tell the story
From reproductive rights to climate change to Big Tech, The Independent is on the ground when the story is developing. Whether it's investigating the financials of Elon Musk's pro-Trump PAC or producing our latest documentary, 'The A Word', which shines a light on the American women fighting for reproductive rights, we know how important it is to parse out the facts from the messaging.
At such a critical moment in US history, we need reporters on the ground. Your donation allows us to keep sending journalists to speak to both sides of the story.
The Independent is trusted by Americans across the entire political spectrum. And unlike many other quality news outlets, we choose not to lock Americans out of our reporting and analysis with paywalls. We believe quality journalism should be available to everyone, paid for by those who can afford it.
Your support makes all the difference.Why are we asking this now?
Aids has killed more than 30 million people in the last quarter century and is continuing to cause around two million deaths a year. Yet as a predominantly sexually transmitted disease, it is possible to avoid it by taking precautions – using condoms and avoiding multiple sexual partners.
In this respect it is unlike infectious diseases such as flu, which it is virtually impossible to avoid. At the International Aids Conference, which opened in Mexico City this week, experts called for a new focus on HIV prevention through behaviour change. Geoffrey Garnett, of Imperial College, London, told the conference that combining different approaches could "dramatically alter the future spread" of the disease.
How much does the Aids impact vary around the world?
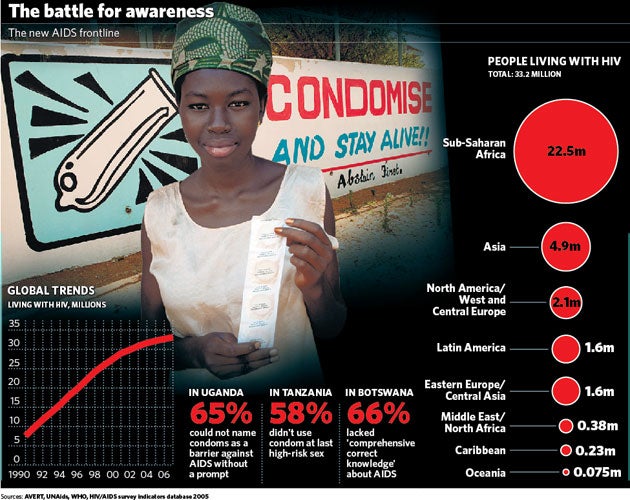
The Aids epidemic is different in Africa than the rest of the world. Where once it was seen as a risk to populations everywhere, it is now recognised that, outside sub-Saharan Africa, HIV is largely confined to high-risk groups including injecting drug users, sex workers and men who have sex with men.
Sub-Saharan Africa is the only part of the world where there is a generalised epidemic that has spread through the heterosexual population. As a result, over two thirds (67 per cent) of all people infected with HIV live in sub-Saharan Africa. Experts do not now expect HIV to spread extensively into heterosexual populations outside Africa.
How easy is it to become infected with HIV through sex?
Not as easy as people think. On average, transmission of the virus occurs in one in 1,000 acts of sexual intercourse with an HIV infected person. For a couple having regular sex, one of whom is infected, the chances of passing the virus are around 8 per cent a year. However, the risks vary widely according to the circumstances and can be as high as one in three acts of sexual intercourse. They are dramatically higher when ulcerative sexually transmitted diseases are present, in anal sex and when the infected partner is at the point in their illness when they are most infectious.
Why is the epidemic so bad in Africa?
No one is really sure. Recent research suggested that there may be a genetic susceptibility that accounts for higher rates of infection among black Africans. Aids deniers, such as Thabo Mbeki, the President of South Africa, have suggested that poverty rather than HIV is the root of Aids in the continent, weakening immune systems through malnutrition. But this ignores evidence showing that HIV infection is higher among the better off, such as teachers, perhaps because they (especially men) can afford to have more sexual partners.
Low rates of circumcision, which is protective, and high rates of genital herpes, which causes ulcers through which the virus can enter the body, have also contributed to Africa's epidemic.
Do African people have more sex?
There is no evidence that they do – though obtaining a definitive answer would be difficult. Epidemiologists believe that, while there are large differences in levels of sexual activity within populations – the young are more active than the old, and city dwellers more active than rural dwellers (because they have access to more partners) – there are likely to be only small differences between populations.
So why theheterosexual spread of the disease in Africa?
It is the question Aids experts are asked most often, but have the greatest difficulty in answering. The answer is likely to be a combination of factors – more commercial sex workers, more ulcerative sexually transmitted disease, a young population, and concurrent sexual partnerships.
It is this last factor that is thought to be key. Even though there is no evidence that Africans have more sex, research suggests there is a higher frequency of overlapping sexual partnerships, creating sexual networks that, from an epidemiological point of view, are more efficient at spreading infection. It may be that serial monogamy, as practised in the UK and many other countries, is an effective barrier to the spread of HIV. It was this issue – of the need to encourage monogamous relationships in Africa – that former US president Bill Clinton highlighted in a BBC interview yesterday.
Aren't condoms the answer?
Yes – if men can be persuaded to use them, and the latest biannual report from UNAIDS, published last week, suggests that condom use is increasing and new HIV infections are falling, partly as a result.
In addition, in seven badly affected countries – Burkina Faso, Cameroon, Ethiopia, Ghana, Malawi, Uganda, and Zambia – young people appear to be waiting longer before starting to have sex. But though new infections dropped from three million to 2.7 million last year, the rate of decline is not fast enough. For every two people that started on treatment with anti-retroviral drugs last year, five become newly infected, amounting to 7,000 a day.
How else should behaviour change?
Injecting drug users are among the groups at highest risk of HIV because sticking a needle that has just been used by someone else into a vein is the most efficient way of transmitting the virus. Efforts at "harm reduction", for example by setting up needle exchange schemes where drug addicts can get clean needles in exchange for dirty ones with no questions asked, should be a key element of any HIV prevention strategy. But only a third of countries have implemented harm reduction programmes. It is a cornerstone of HIV development programmes supported by Australia but gets no support from the US or Sweden.
What's the main area of concern in the West?
One of the danger areas is transmission of the virus among men who have sex with men. This is not declining and in some places has increased. In the developing world, too, it has been neglected, but when researchers look for it, they find it. In the UK, after an initial decline in sexually transmitted diseases among men who have sex with men, infection rates are rising again.
Experts say it is an area that needs a more rigorous approach in the future. In countries where this is the main mode of transmission, less than a quarter of the men involved had access to prevention based on condom use.
So is the Aids argument being won?
Yes...
*New HIV infections are falling – from three million to 2.7 million last year
*Condom use is increasing and the age of first sex is rising in some parts of Africa
*Injecting drug users will avoid sharing dirty needles – if given access to clean ones
No...
*Despite the recent fall, there are 7,000 new HIV infections a day – too many to treat
*Changing sexual habits over the long term is notoriously difficult to achieve
*Other measures, such as circumcision, will be necessary to beat the disease
Join our commenting forum
Join thought-provoking conversations, follow other Independent readers and see their replies
0Comments